By Jonathan Jackson, PhD
I am a cognitive neuroscientist on faculty in the Neurology department at Massachusetts General Hospital (MGH). I research the early detection of Alzheimer’s disease in a human research laboratory in Boston, Massachusetts. Working in a hospital may sound wildly different from running a lab in a university, but it is actually a lot more similar than you might think. If you’re considering a research career, please read on; this may be an attractive option that you may not have considered.
In many ways I am a traditional academic. I’m on the tenure track at Harvard Medical School (HMS), for example. I am required to generate, communicate, and evaluate research through peer-reviewed publications. We hold weekly lab meetings to discuss (read: argue about) the latest research findings from our own and other Alzheimer’s labs. There are dozens of committees at MGH that I may join in order to fulfill service obligations. I work with brilliant colleagues on complex problems. You won’t find patient beds on our floor; instead, we work in a mix of traditional cubicles and offices that you’d find at any university. Overall, the environment I work in, and career goals I strive toward wouldn’t feel out of place in any university setting.
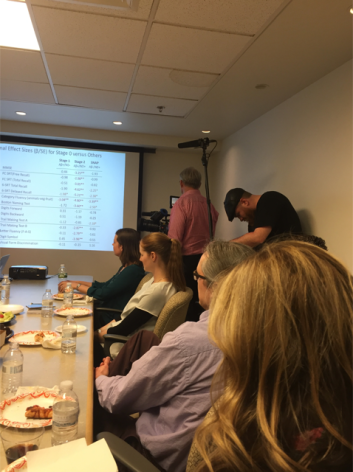
Like many labs, we have regular meetings to discuss the latest findings from our research. However, sometimes our meetings are attended by a film crew hoping to learn about breakthroughs in the fight against Alzheimer’s disease!
However, there are also a number of striking differences that might make working at HMS / MGH more (or less!) appealing for those looking to develop research careers outside of the typical college or university campus.
The biggest difference is in how my laboratory is structured. First of all, there aren’t any graduate students (or medical students)! Instead, we have more than 20 doctoral-level (PhDs, MDs, and PsyDs) individuals and 15 (mostly post-baccalaureate) research assistants performing full-time research around a large NIH-funded program project grant and several satellite grants. Collectively, we run the Harvard Aging Brain Study, a large prospective cohort of 400 older adults. Although many of us are on the tenure track, have obtained our own NIH or foundation funding, and have largely independent research careers, more senior lab members will mentor the younger ones, and tend to have more influence in how the overarching study is tweaked and conducted. Physicians and clinicians within the group divide their time between research and clinical practice (i.e., seeing patients), while researchers purely focus on the advancement of science.
The lab is loosely divided three into semi-autonomous sections: 1) neuropsychology, which deals with the clinical assessment of healthy aging and dementia using paper-and-pencil tests and semi-structured clinical interviews, 2) neuroimaging, which includes development of many novel MRI and PET technologies, and 3) our clinical trials unit, the Center for Alzheimer Research and Treatment, which is located at Brigham & Women’s Hospital. At any given moment, the clinical trials unit is testing 8-10 potential treatments for Alzheimer’s disease, usually in Phase III clinical trials. Each section is run by a tenured professor / physician, and while most researchers stay within a domain, there are a few people like me who cut across all three sections, and work to translate basic research from our lab to our clinic. Yes, this means I have three offices in three different locations around Boston!

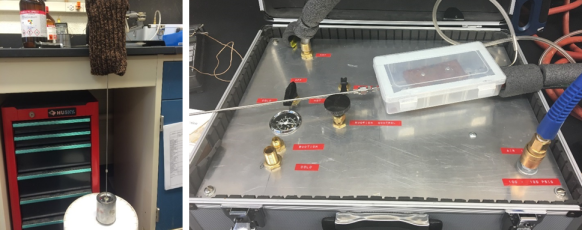
Interior photo of MGH’s Building 149 at the Charlestown Navy Yard, where much of our research on healthy older adults is conducted.
Beyond the lab itself, there are other major differences between my career and that of the typical academic. Another big, big difference is that because there are no students, there is no teaching (and alas, no summer breaks)! Many academics in the university model must negotiate and balance teaching alongside of research. Here at HMS, tenure and promotion is based purely on clinical work, research productivity, and hospital / community service. Less-formal and informal teaching opportunities are still abundant, however. For example, I have convened two statistical courses this year within my lab, one for the research assistants and one for the doctoral researchers. And through the Harvard Catalyst system, it is also possible to take or teach courses on an enormous variety of subjects, including career-oriented options like lab management and budgeting, advanced grantwriting, and research development.
The tenure track at HMS is also somewhat different from the university model. There is an added level below the assistant professor rank, called Instructor. Postdoctoral fellows tend to apply to the Instructor rank when they intend to remain with the lab they work in as a permanent option, rather than staying postdocs forever. Instructors tend to have much more stability than postdocs, receive higher salaries, and have access to a broader suite of resources at Harvard and MGH.
The path to tenure has also been tweaked. Although the main Harvard University campus was once notorious for making the path to tenure extremely difficult, there are very clear, achievable guidelines for the process at HMS. There is no tenure clock, meaning you can stay at the Instructor rank – or any other – as long as you’d like before applying to the next-higher level. This comes with a clear risk over typical university positions, though: The downside is that with no clock, there is no guaranteed salary support. This is often called a “soft money” position, and means that your salary comes exclusively through the grants you write and receive. This can be stressful when the funding climate becomes very competitive, but both HMS and MGH have several internal grant awards designed for funding gaps. So the reality is that although the money is soft, many researchers can go 4-5 years without a successful external grant before salary support becomes a problem.
All in all, I am very glad to be developing my career in a hospital setting, and particularly at HMS / MGH. This is because my job has far more flexibility than what I’d be doing in a university setting. Research can and must remain a primary focus, but beyond that, it’s really up to me. I can teach or not, I can see patients or not, I can set up my own mini-lab within my research group or not. I can take on some of these things temporarily and then give them up later without major consequences. Some people work within my research group indefinitely, while others enter the job market after a few years. While there’s a strong incentive to write and receive grants, HMS / MGH have developed a strong support structure to make it easier to succeed in grantwriting. This is supplemented by the support structure within my lab for grants and high-impact research.

We wear many hats in my hospital laboratory. Here is the team that runs the Center for Alzheimer Research and Treatment, our clinical trials arm located at Brigham & Women’s Hospital.
All this adds up to the best part of my career: work-life balance. We definitely work hard, but it’s possible to take many weekends and evenings off to spend with family and loved ones. While the exact number of hours per week varies by personality, life stage, and whether a grant is coming due, nearly everyone in my lab has been able to find their optimal work schedule. I believe that this contributes to the strong diversity in my lab, which is made up of many parents and is about 70% female, including at the most senior levels of our group.
Things at HMS / MGH aren’t perfect, of course, but for those who wish for research options outside of the traditional lab-and-university environment, it’s a great “alternative” career with only a few tradeoffs from the standard academic model. Please leave questions and comments below – I’d be happy to expand on the details of my day-to-day.


 By Sarah McAnulty (@SarahMackAttack), a doctoral candidate in the Nyholm lab (Department of Molecular and Cell Biology, University of Connecticut)
By Sarah McAnulty (@SarahMackAttack), a doctoral candidate in the Nyholm lab (Department of Molecular and Cell Biology, University of Connecticut)